|
Philip van der Wel Administrator Posts: 145
1/15/2016
|
Philip van der WelAdministrator Posts: 145
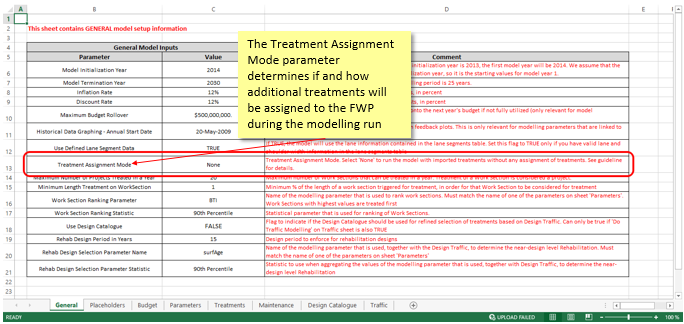
On the General worksheet in the Deterioration Model Setup (DMS) file you must determine whether the model will assign treatments or run with imported treatments; this is done via the Treatment Assignment Mode parameter.
The approach to assigning or triggering treatments is a key part of your Deterioration Model Setup. JunoViewer provides several approaches to assigning treatments.
The possible values for Treatment Assignment Mode are outlined below (please note that most of these modes were previously named differently and were changed to more descriptive values. The older mode names are now deprecated but can still be used). To prevent typing errors, it is suggested that you copy and paste the names shown in Bold below into your DMS file:
- None: Run the model with imported treatments without assigning any treatments.
- Ungrouped, Ranked, Cost-Constrained: Allocate treatments based on the chosen ranking parameter (e.g. Benefit Cost Ratio) without taking into account segment groupings or lanes. Assigned treatments are constrained based on a specified budget. The budget can be either monolithic (a single budget figure for each year), or categorized (a separate annual budget for each treatment category); [Previously called "Basic Ranking"]
- Ungrouped, Ranked, Quantity-Constrained: Allocate treatments based on the chosen ranking parameter (e.g. Benefit Cost Ratio), without taking into account segment groupings or lanes. Assigned treatments are constrained based on specified quantities for each category of treatment. Note that for this mode, ranking is done on on an individual segment basis (i.e. not on a Grouped Basis); [Previously called "Treatment Quantity Constrained"]
- Ungrouped, Ranked, KPI-constrained: Allocate treatments based on ranking which automatically related to the effect of triggered treatments on the KPIs. For details on how the KPI ranking works for this model, please see this post. This model does not take into account segment groupings or lanes. Assigned treatments are constrained based on set of Key-Performance-Indicators and optionally a specified budget. The budget can be either monolithic (a single budget figure for each year), or categorized (a separate annual budget for each treatment category);
- Ungrouped, NPV-Optimized, Cost-Constrained: This model will allocate treatments based on a full Benefit-Cost Analysis of all possible strategies, coupled with optimized project selection to maximize benefits across the network. This method requires you to define a Cost of Use function as one of your model parameters, in order for a "Do Nothing" scenario to be assessed. Optimization is based on a budget constraint, using either a monolithic budget (a single budget figure for each year), or categorized (a separate annual budget for each treatment category); Note that - for identifying projects on the Pareto Front, the Incremental Benefit Cost Ratio method is always used, regardless of the treatment assignment mode. However, when it comes to selecting the optimal project on the Pareto Front, you can either favour projects with high benefits (maximise NPV - this method) or you can favour projects with higher benefit cost ratios (maximise BCR, see next bullet). For more information on this topic, please refer to this post and its related links. [this method was previously called "NPV - Cost Optimized"].
- Ungrouped, MaxBCR-Optimized, Cost-Constrained: Allocate treatments based on a full Benefit-Cost Analysis of all possible strategies, coupled with optimized project selection to maximize Benefit-Cost Ratio across the network. This method will strive to seek the lowest cost solution to maximize benefits. It will tend to favour lower cost treatments. This method requires you to define a Cost of Use function as one of your model parameters, in order for a "Do Nothing" scenario to be assessed. Optimization is based on a budget constraint, using either a monolithic budget (a single budget figure for each year), or categorized (a separate annual budget for each treatment category); See this link for details on deficiencies when selecting projects based on BCR;
- Grouped, Ranked, Cost-Constrained: Allocate treatments in work section groups. In this mode, the ranking parameter is calculated for each segment group and segment groups are then treated as a whole when the group is selected for treatment. Treatments applied to segments within the group can differ based on individual segment condition, but the time of treatment will be the same for all segments in the group. This method is often used to plan treatments on freeways where all lanes need to be treated in the same year, but with different treatment types. Note that this model can be used with-or-without Key Performance Indicator (KPI) constraints. Details on how to use this model with KPI constraints can be found in this post.
- Grouped, Ranked, Cost-Constrained, Slow Lane Governs: Allocate treatments in work section groups, but with treatments only triggered on slow lane segments (i.e. those where the lane code ends with “1”, e.g. “L1”, “R1”). Treatments for fast lane segments will be allocated according to the treatment code assigned to the “Fast Lane Treatment” property for the slow lane treatment on the “Treatments” sheet. [Previously called "Work Section – Slow Lane Governs"]
Other treatments assignment modes can be programmed based on the requirements of your network; contact Lonrix Ltd to discuss your options.
For information on the other general options required to run the model, please refer to this post.
The following Treatment Assignment Mode NAMES have been deprecated:
- Ungrouped, IBCR-Optimized, Cost-Constrained: This method is mathematically the same as the NPV method (see above) and will always give the same results. Note that it is simply the label/name of the method that has been deprecated. We have decided to retain the NPV label instead of the IBCR label, although both methods will give the same results. Also note that - for identifying projects on the Pareto Front, the Incremental Benefit Cost Ratio method is always used, regardless of the treatment assignment mode. However, when it comes to selecting the optimal project on the Pareto Front, you can either favour projects with high benefits (maximise NPV) or you can favour projects with higher benefit cost ratios (maximise BCR). For more information on this topic, please refer to this post and its related links. Since this method name is deprecated, please use: "Ungrouped, NPV-Optimized, Cost-Constrained" instead.
edited by Fritz on 9/22/2022
|